
A brief review of equinus deformity
Children with cerebral palsy (CP) often exhibit equinus foot deformity during gait. This is due to both neurological (co-contraction of the agonists and antagonists, reduced central control of the dorsiflexors, overactivity of the plantarflexors) and muscular (increased stiffness, reduced length and extensibility, reduced sarcomere growth, and consequent weakness) causes.
However, the relationships between the underlying causes and their combined role in the onset of foot deformity are still unclear.
New studies and collaborations
Andrea Merlo has recently published a new article in collaboration with neurological disorders specialists from the Timone Children’s Hospital in Marseille (FR), the University Children’s Hospital in Basel (CH), and the University Hospital of Creteil (FR).
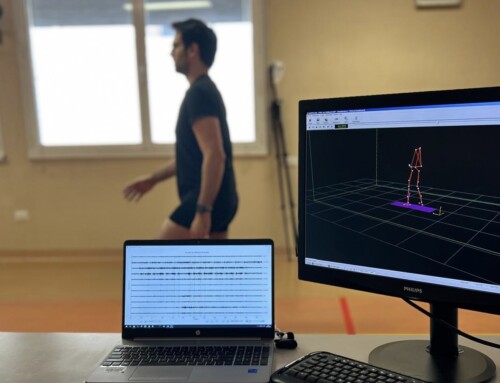
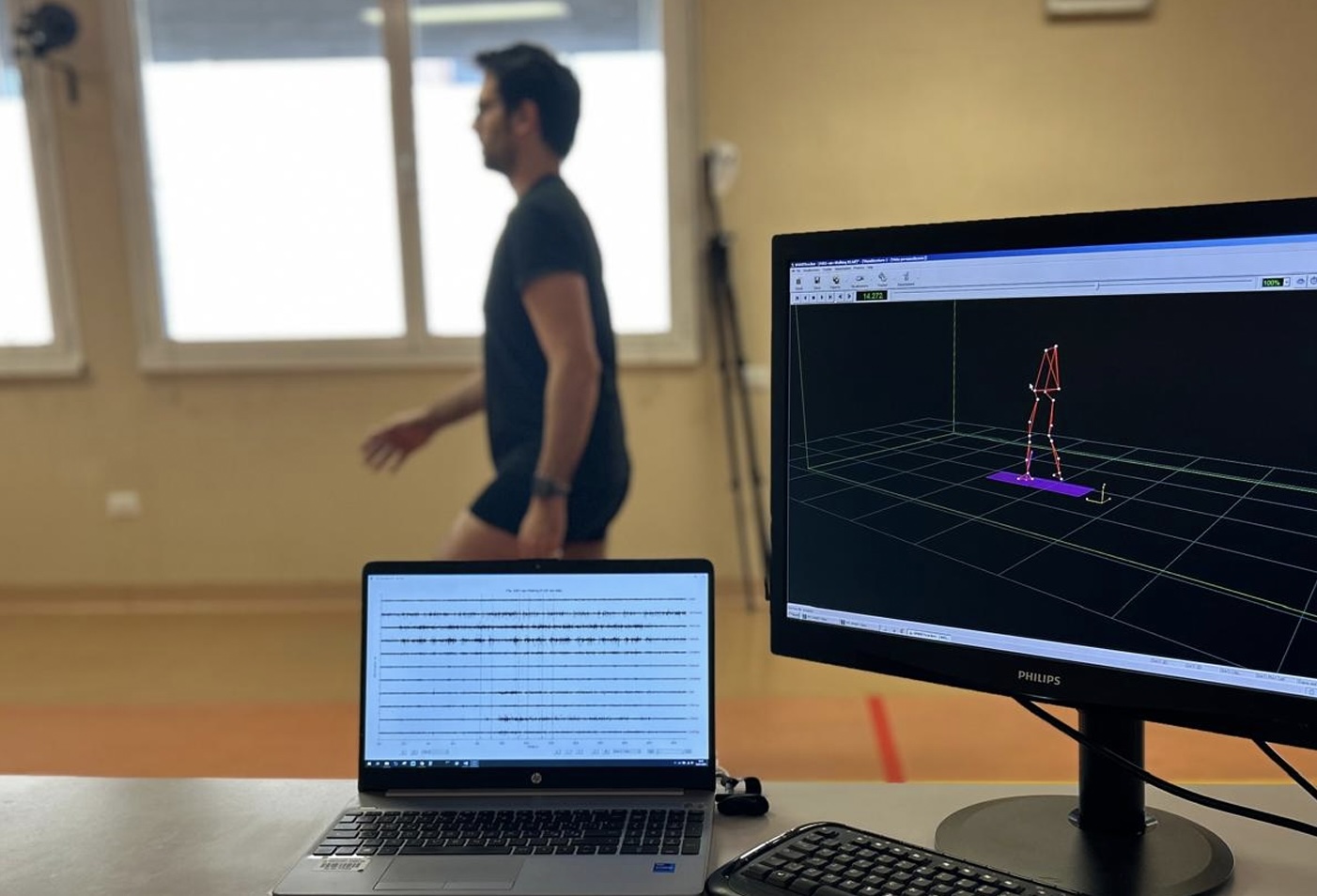
The team analyzed about thirty children under six and registered ankle joint ranges of motion, focusing on the soleus alone and the gastrocnemius-soleus complex. Dynamic EMG of the gastrocnemius medialis, the peroneus longus, and the tibialis anterior, and gait video observation were also performed.
The Five-Step Assessment method for spastic paresis was used.
First step: weighting central and peripheral factors
The study aimed to quantify the peripheral and central components leading to equinus foot deformity in CP children.
Authors found reduced extensibility of the triceps complex that decreased as children’s age increased, suggesting a progressive deterioration of muscle length with growth. Moreover, less extensible muscles were found to have a lower threshold for the spastic stretch response, maybe due to an increased sensitivity of the neuromuscular spindles.
Focusing on agonist muscles, dorsiflexion was difficult to perform in most samples due to antagonist co-contraction, poor selective motor control, and inhibition of the tibialis anterior. This confirms what had already been seen in adult neurological populations: a vicious cycle of soft tissue stiffness and muscle overactivity leads to altered agonist-antagonist synergies in children.

Second step: the role of the peroneus longus
The study’s second aim was to deepen the role of the peroneus longus in the development of the equinovalgus foot deformity during gait.
This muscle was more active than the gastrocnemius during the swing phase, causing the plantarflexion deviation, even with the tibialis anterior trying to counteract its action. This pattern reduced with age, suggesting some improvement in selective motor control.
This study found age-related changes in CP children: muscle composition tends to worsen while motor control improves during aging.
The full-text article can be found here.
These findings represent a great starting point for designing rehabilitation plans specific for CP children, which were demonstrated to be different from neurological adults in the development of deformities.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}